Issue Category: Substance Misuse and Mental Health
Combined Deaths from Alcohol, Drugs and Suicide Declined by 16% in 2024
New Report Highlights How Progress is at Risk Amid Federal Workforce and Funding Cuts; Special Feature on Suicide Sheds Light on Disparities
(Washington, D.C. – June 2, 2026) – The death rate from alcohol-induced, drug overdose, and suicide causes were each down significantly in the United States in 2024 for the first time since 1999 (when datasets were initially published), and provisional data for 2025 signals this positive trend has continued.
A new report from Trust for America’s Health (TFAH) explores what’s behind these recent downward trends, which demographic groups are still experiencing high rates of death from these causes, and how federal workforce and funding cuts are putting progress at risk.
Pain in the Nation 2026: The Epidemics of Alcohol, Drug, and Suicide Deaths, which examines data from the Centers for Disease Control and Prevention (CDC) and other federal sources, finds that the combined age-adjusted rate of deaths from alcohol, drugs, and suicide declined by 16 percent in 2024, building on a decrease of 4 percent in 2023. Specifically, alcohol-induced mortality declined by 4 percent, drug overdose mortality by 26 percent, and suicide mortality by 3 percent.
Most states saw improvements in their combined rates as well: 45 states and the District of Columbia had lower rates compared to 2023, four states had higher rates (Iowa, North Dakota, South Dakota, and Wyoming), and one state stayed the same (Nebraska) in 2024.
Cuts to public health workforce and funding, as well as uncertainty surrounding long-standing federal programs and grants, significantly threaten this progress. For example, the CDC’s National Center for Injury Prevention and Control (Injury Center), Substance Abuse and Mental Health Services Administration (SAMHSA), Veterans Affairs health care staff, and 988 Suicide and Crisis Lifeline’s LGBTQ+ youth services all experienced cuts or eliminations, despite the critical role these programs have in reducing deaths from these causes.
“Sustaining and building on recent progress requires the federal government to invest even more in programs that reduce and prevent harm—not cut them—while also investing in the skilled workforce and modern data systems necessary to deliver and evaluate those programs effectively,” said Dr. J. Nadine Gracia, President and CEO of TFAH. “We are also seeing specific groups of people not experiencing the same progress, especially when it comes to deaths from suicide, meaning we need to do even more to build strong policies and programs that help to improve everyone’s mental health and well-being,”
The report examines the strategies, policies, and programs that have helped drive the recent decline in mortality, including:
- Creating and sustaining new federal programs and infrastructure, including prevention grants such as SAMHSA’s Garrett Lee Smith program (2004) and the CDC’s Comprehensive Suicide Prevention program (2020) and Preventing Adverse Childhood Experiences through Data to Action (2023).
- Investments in data systems, like CDC’s Overdose Data to Action and the National Violent Death Reporting System, have allowed health officials to track emerging trends by geographic, demographic, and drug type metrics to guide local, state, and national responses and to prevent overdoses and deaths in real time in communities in need.
- A growing focus on the drivers of substance misuse and poor mental health through prevention and early intervention policies, including improving social, environmental, and economic conditions; expanding resilience programs in schools; and increasing access to social and mental health services for children and families.
Pain in the Nation includes a special feature on suicide, which was the 10th leading cause of death in 2024 and the second leading cause of death for people ages 10–14, 15–24, and 25–35. Key findings related to suicide include:
- Suicide rates across nearly all racial and ethnic groups were lower in 2024, after peaks in 2022 or 2023. Despite this progress, American Indian and Alaska Native people consistently have the highest suicide rate of any race/ethnicity.
- Historically, Black youth have had relatively low suicide mortality rates compared to their peers, but rates have risen at an alarming pace in recent decades, increasing 144 percent from 2007 to 2020.
- Suicide rates are higher in rural areas compared with urban areas and have increased at a faster rate over the last two decades. The most recent data available, from 2022, show that rural areas had a suicide rate 41 percent higher than urban areas.
- While the rate of suicide deaths is unknown for LGBTQ populations, research consistently find higher rates of mental health issues, substance use, and suicidal behaviors for LGBTQ individuals compared with heterosexual individuals.
The report also calls for a sustained commitment to primary prevention programs and investments, and includes recommendations on actions the Administration, Congress and federal agencies should take, such as:
- Investing in prevention and conditions that promote health
- Spend behavioral health funds and carry out investments as directed by Congress.
- Provide robust funding for CDC’s Injury Center and maintain the vital workforce necessary to fulfill the Center’s activities.
- Support policies and programs that reduce adverse childhood experiences and the impact of trauma and promote positive childhood experiences.
- Reducing overdose risk and access to lethal means of suicide
- Support policies to reduce overdose and bloodborne infection.
- Support efforts to limit access to lethal means of suicide, such as safe storage of medications and firearms.
- Transforming the mental health and substance use prevention system
- Maintain SAMHSA’s funding and critical workforce and bolster the continuum of crisis intervention programs and supports, such as the 988 Suicide and Crisis Lifeline.
- Restore Medicaid funding and eligibility to prevent losses in mental health and substance use healthcare.
- Promote equity in mental health, with a specialized workforce and targeted services to reduce disparities in access and outcome.
Read the full report
Pain in the Nation 2026: the Epidemics of Alcohol, Drug, and Suicide Deaths

Letter in Support of Primary Prevention Funding Programs that Promote Community Well-Being (December 2025)
Public Health Leaders’ Joint Statement in Response to the Attack on CDC
(Washington, DC – August 14, 2025) – In response to the horrific shooting that occurred on Friday, August 8, targeting the Centers for Disease Control and Prevention (CDC), the public health community stands in solidarity with our CDC colleagues. We denounce acts of harassment, terror, and violence against the public health workforce.
Our hearts break for the family of police officer David Rose who lost his life protecting his community.
Two hundred bullets struck and caused damage to six federal buildings and over 500 rounds were fired at the CDC campus. We are saddened, alarmed, and deeply concerned about the health and safety of our colleagues. The shooting was an attack on an American workplace and on the people and infrastructure that keep us all healthy and safe.
We are committed to working together to support our nation’s dedicated public servants who comprise the public health workforce and call on others to do the same. It is critical to the health of all communities that CDC and all people working in public health across the country are able to continue to make their invaluable contributions to advancing health and well-being without the fear of harassment or violence.
People choosing public health as a profession are committed to advancing our nation’s health and recognize that good health in every community benefits everyone. It is our hope that all Americans will stand with us to support the vital role that CDC and the entire public health workforce play in supporting safety and well-being in every community. Their expertise and commitment to advancing health deserves all Americans’ unwavering support.
American College of Epidemiology
American College of Epidemiology Research and Education Foundation
American Public Health Association
Association of Maternal and Child Health Programs
Association of Public Health Nurses
Association of State and Territorial Dental Directors
Association of State and Territorial Health Officials
Association of State and Territorial Public Health Social Workers
Association of Public Health Laboratories
Association of Schools and Programs of Public Health
Big Cities Health Coalition
CDC Foundation
Council of State and Territorial Epidemiologists
de Beaumont Foundation
National Association of Chronic Disease Directors
National Association of County and City Health Officials
National Association of State Emergency Medical Services Officials
National Network of Public Health Institutes
Prevention Institute
Public Health Accreditation Board
Safe States Alliance
The Kresge Foundation
Trust for America’s Health



![]()
![]()






![]()








Marking Three Years of 988 Suicide and Crisis Lifeline Support for People in Need

Since its launch in July 2022, the 988 Suicide and Crisis Lifeline has responded to millions of individuals and has provided immediate support to callers who are in crisis. Still, recent and proposed cuts to the Substance Abuse and Mental Health Services Administration (SAMHSA) and 988 services and the lack of state funding could leave individuals in need or others with fewer options for life-saving help.
The national 988 Suicide and Crisis Lifeline has answered more than 14 million calls, texts, and chats since it was introduced. Call volume to the Lifeline in the first two years of its existence was up 95 percent nationally as compared to calls to the 1-800 system it replaced. In addition, call answer rates have improved and wait times have been reduced.
Still, recent major cuts to agency workforce and a recent decision to end specialized services through 988 for LGBTQIA+ youth and young adults is poised to set that progress back and could have dire consequences.
Brief History
The 988 Suicide and Crisis Lifeline was established by Congress in 2020 and launched officially in 2022 in an effort to enhance the nation’s crisis care system. Established by Congress, 988 was designed to make the previous seven-digit 1-800 suicide prevention lifeline more accessible by creating an easy to remember call number and adding a text option. In 2024, calls and texts began being routed to local crisis centers based on geographic location instead of area codes to help connect users with faster and local support.
In addition, the 988 Lifeline has included specialized support for military veterans, LGTBQIA+ youth, and Spanish-language speakers. To address the disproportionate rates of suicide among American Indian and Alaska Native populations and provide culturally and trauma informed crisis services, the state of Washington offers specialized care for Washington’s American Indian and Alaska Native communities.
People seeking assistance through the 988 Lifeline are able to call, text, and chat through the website with trained professionals at 988 call centers. Counselors either counsel callers through their crisis or direct individuals to acute care in their community.
Research from the American Association of Suicidology found that two-thirds of the people who had suicidal thoughts and reached out via the Lifeline’s online chat reported that the correspondence had been helpful, and 45% reported being less suicidal.
The Need and Demand for the Crisis Lifeline
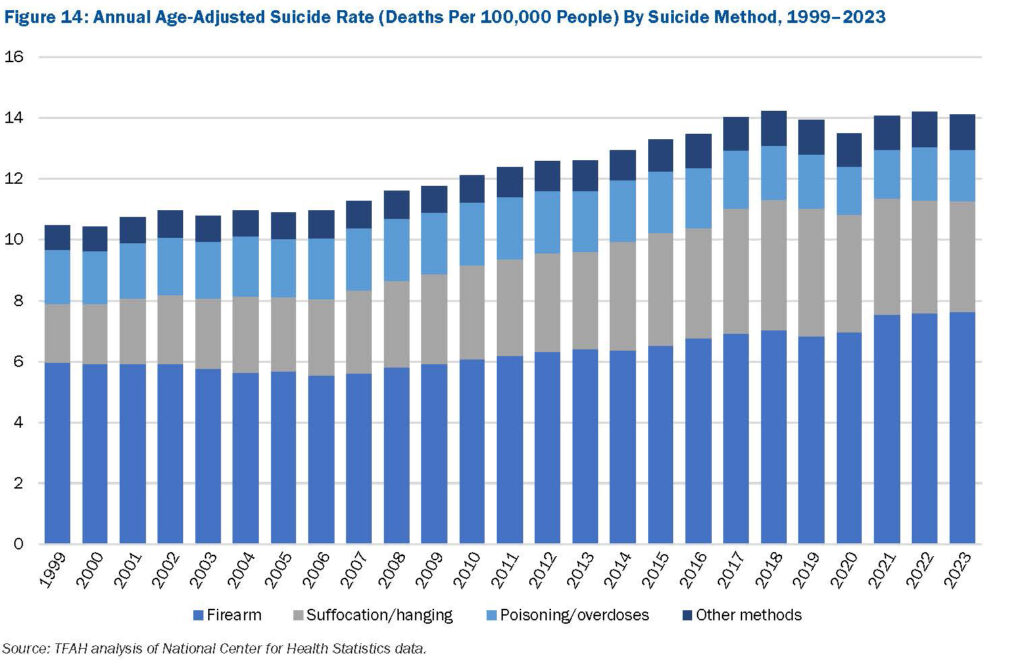
 According to the latest edition of Trust for America’s Health’s Pain in the Nation: The Epidemics of Alcohol, Drug, and Suicide Deaths report, nearly 50,000 Americans of all ages died by suicide in 2023. Although there has been some fluctuation over the past few years, suicide rates have generally been on the rise since 1999. Nearly a half million people died from died by suicide in the U.S. from 2014 to 2023.
According to the latest edition of Trust for America’s Health’s Pain in the Nation: The Epidemics of Alcohol, Drug, and Suicide Deaths report, nearly 50,000 Americans of all ages died by suicide in 2023. Although there has been some fluctuation over the past few years, suicide rates have generally been on the rise since 1999. Nearly a half million people died from died by suicide in the U.S. from 2014 to 2023.
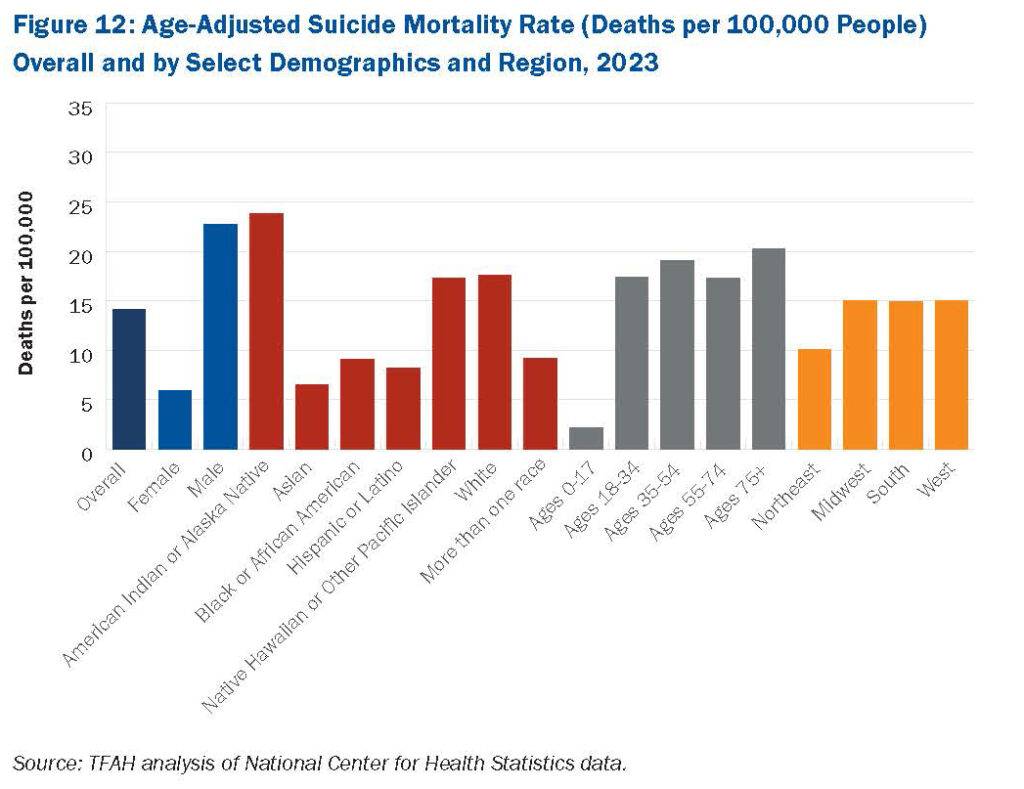
 Some of the highest age-adjusted suicide rates are seen in males and adults ages 75 and older. Suicide rates in rural areas are consistently and significantly higher than urban areas, research shows as well.
Some of the highest age-adjusted suicide rates are seen in males and adults ages 75 and older. Suicide rates in rural areas are consistently and significantly higher than urban areas, research shows as well.
To turn the tide, TFAH urges federal and state policymakers to transform the nation’s mental health and substance use prevention system, in part by strengthening the continuum of crisis intervention supports and programs. TFAH also urges federal agencies to do more to encourage and make people feel more comfortable seeking help with mental health issues, for example by promoting culturally appropriate messaging on mental health screening and treatment to reduce stigma. The 988 Lifeline provides a pathway for states and local communities to implement those recommendations.
Federal and State Support Needs to be Sustained and Increased
The 988 Lifeline is funded primarily through federal funding and is administered by the Substance Abuse and Mental Health Services Administration (SAMHSA). Some states provide additional funding support through their annual budgets and/or telecommunications fees. To date, 16 states are providing funding for their 988 networks. Unfortunately, there are ongoing threats to funding for 988 and suicide prevention services. In March 2025, the Department of Health and Human Services (HHS) announced they would be clawing back $1 billion in SAMHSA funds, including mental health grants many states were applying to 988 suicide lifelines and crisis services. Litigation is putting this clawback on hold in some states. In addition, reductions in force at SAMHSA and the President’s FY 26 Budget Request which proposes to eliminate SAMHSA and significantly reduce mental health programs and funding, could undo progress communities are making in addressing suicide, mental health, and substance use crises.
Where Do We Go From Here?
To continue to support the nation’s crisis services, the following action steps are needed:
- Congress and the Administration should strengthen the 988 Suicide and Crisis Lifeline by maintaining SAMHSA funding for the Lifeline and by restoring the workforce devoted to these services. SAMHSA should also retain the 988 Lifeline’s specialized services, including specialized support for LGBTQIA+ youth and Spanish-language services.
- Congress should also pass the 9-8-8 Implementation Act, which would authorize funding for crisis call centers to purchase or upgrade call center technology, hire and train call center staff, and improve call center operations.
- More states should dedicate funding for the 988 Lifeline and more investments should be made to improve geo-location technology so people that need help are directed to services in their community.
Pain in the Nation 2025: The Epidemics of Alcohol, Drug, and Suicide Deaths

Watch Trust for America’s Health’s (TFAH) for a national webinar and congressional briefing on our recently released report, Pain in the Nation 2025: The Epidemics of Alcohol, Drug, and Suicide Deaths.
TFAH’s Pain in the Nation 2025 report found that over 200,000 Americans died from alcohol, drugs, and suicide in 2023. While this marks a decline from 2022, deaths remain more than double what they were two decades ago. The report highlights improvements in alcohol and drug-related mortality, but disparities persist. Only white Americans saw a drop in overdose deaths, and rates of such deaths remained highest in communities of color. Furthermore, while the reported data represents real progress, current and potential federal funding cuts, public health workforce reductions, and proposed federal agency reorganizations could undermine it.
The briefing included time for Q&A from the audience.
Deaths Due to Drug Overdose and Alcohol Are Down Nationally, But Progress is Uneven Across Population Groups and at Risk Due to Cuts in Federal Health Programs
How can progress be sustained and extended to all communities?
(Washington, D.C. – May 28, 2025) – Deaths due to drug overdose and alcohol misuse were down in the United States in 2023 according to Centers for Disease Control and Prevention (CDC) data and newly released CDC 2024 provisional data predict an unprecedented 27 percent one year drop in overdose deaths. These reductions are encouraging and were likely related to a number of factors including investments in primary prevention, mental health, harm reduction, and overdose prevention programs. However, current and proposed federal budget cuts, public health workforce reductions, and proposed federal agency reorganizations are likely to undermine this progress, according to a new report.
Pain in the Nation 2025: The Epidemics of Alcohol, Drug, and Suicide Deaths, released today by Trust for America’s Health, reports that the combined number of deaths from alcohol, drugs, and suicide in the United States declined in 2023 for the second straight year—after two decades in which such deaths increased at an alarming pace. Still over 200,000 Americans died due to alcohol, drug overdose, or suicide in 2023, twice the rate of such deaths 20 years ago.
The new data highlight the value of investment in mental health and substance use prevention programs – such as ensuring adequate mental health, substance use disorder, and crisis intervention services, access to overdose reversal drugs, and investing in children’s mental health and resilience. The data however also show that much more needs to be done to ensure that the progress against alcohol, drug overdose, and suicide deaths is sustained and that reductions in such deaths are occurring in every community and among all population groups.
“Data show that decades of investment and capacity building in substance use prevention, harm reduction programs, and mental health services have helped reduce associated deaths. The challenge now is to build on these investments and sustain this progress. These programs save lives; their funding should not be cut,” said J. Nadine Gracia, M.D., MSCE, President and CEO of Trust for America’s Health.
Drug overdose rates are declining but still at tragic levels.
In 2023, 105,007 Americans across died from drug overdoses. After precipitous increases in the rate of drug overdose deaths in 2020 and 2021, the 2022 overall overdose mortality rate was virtually unchanged and the 2023 mortality rate was 4 percent lower. Provisional mortality data for 2024 show an unprecedented one-year 27 percent decrease in overdose deaths nationally. Seven states (Louisiana, Michigan, New Hampshire, Ohio, Virginia, West Virginia, and Wisconsin) and Washington D.C. saw the greatest reductions, with declines of 35 percent or more in overdose deaths for the year.
According to public health experts, improved data systems which allow for real-time tracking of substance use and its impacts, the expansion and effectiveness of overdose prevention strategies such as programs to ensure access to naloxone, buprenorphine, and drug-checking tools all played a significant role in bringing down mortality rates.
The improvement was, however, not consistent across all population groups or regions of the country. In 2023, white people were the only racial/ethnic population group that experienced a statistically significant decrease in drug overdose deaths; other population groups had nonsignificant changes or increases. Drug overdose death rates in 2023 were highest among American Indian/Alaska Native people (AI/AN) (65.0 deaths per 100,000 people), adults ages 35 to 54 (57.3 deaths per 100,000 people), Black people (48.5 deaths per 100,000 people), and males (45.6 deaths per 100,000 people).
Alcohol-induced deaths are down.
In 2023, 47,938 Americans died from alcohol-induced causes. The overall age-adjusted alcohol-induced mortality rate decreased by 7 percent from 2022 to 2023 (from 13.5 to 12.6 deaths per 100,000 people). This decrease built on a 6 percent reduction the year prior and crossed nearly all demographic and geographic groups, but such deaths still disproportionately impact some groups. Alcohol-induced death rates in 2023 were highest among AI/AN people (61.5 deaths per 100,000 people), adults ages 55 to 74 (32.5 deaths per 100,000 people), adults ages 35 to 54 (20.2 deaths per 100,000 people), and males (18.1 deaths per 100,000 people).
Suicide deaths unchanged.
The U.S. overall suicide mortality rate remained virtually identical from 2022 to 2023 (14.2 and 14.1 deaths per 100,000 people, respectively). In 2023, 49,316 Americans died from suicide. Age-adjusted suicide rates in 2023 were highest among AI/AN people (23.8 deaths per 100,000 people), males (22.7 deaths per 100,000 people), and adults ages 75 and older (20.3 deaths per 100,000 people).
Budget rescissions and future cuts to prevention programs will cost lives.
While these data demonstrate real progress, the public health community is united in its concern about progress reversals due to cutbacks in federal investment in health promotion, crisis intervention, and overdose prevention programs. For example, staff and funding for the CDC Injury Center have been drastically reduced, and the Center is proposed for elimination in the Administration’s budget request for fiscal year (FY) 2026. The Injury Center conducts research and collects data. Approximately 80 percent of its funding goes to states and other entities for prevention of overdoses, suicide, and adverse childhood experiences (ACEs). Additionally, the Substance Abuse and Mental Health Services Administration (SAMHSA) has experienced major staffing reductions including staff working on the 988 Suicide & Crisis Lifeline, and a potential $1.07 billion funding cut for FY 2026. The Administration has proposed folding some remaining SAMHSA and Injury Center programs into a new Administration for a Healthy America. These actions followed the Administration’s claw-back of billions of dollars in public health funding already at work in states and communities across the country, including for suicide prevention.
The Pain in the Nation report calls for sustained investment in prevention and harm reduction programs and includes recommendations on actions federal and state policymakers should take including:
- Protect and bolster investment in public health and behavioral health systems and injury and violence prevention programs to improve mental health and well-being for all Americans.
- Continue to improve programs, like CDC’s Overdose Data to Action, to track emerging trends by geographic, demographic, and drug type metrics to guide local, state, and national responses and to prevent overdoses and deaths in real time.
- Focus on underlying drivers of substance use disorder through early intervention and prevention policies including expanding resiliency and substance use prevention programs in schools and increasing access to social and mental health services for children and families.
- Maximize harm reduction strategies and substance use disorder treatments to reduce overdose risk, and support efforts to limit access to lethal means of suicide.
- Bolster the continuum of crisis intervention programs and expand the mental health and substance use treatment workforce. Build community capacity to ensure access to mental health and substance use treatment for anyone needing such services.
Read the full report
Trust for America’s Health is a nonprofit, nonpartisan public health policy, research, and advocacy organization that promotes optimal health for every person and community and makes the prevention of illness and injury a national priority.
Las muertes a causa de sobredosis por drogas y alcohol disminuyen a nivel país, pero el avance es desigual entre los grupos poblacionales y está en riesgo por los recortes en los programas sanitarios a nivel federal
¿Cómo se puede mantener y ampliar el avance para todas las comunidades?
(Washington, D.C., 28 de mayo de 2025). Las muertes a causa de sobredosis por drogas y abuso de alcohol disminuyeron en los Estados Unidos en 2023, según datos de los Centros para el control y prevención de enfermedades (CDC) y de los últimos datos provisorios publicados por los CDC en 2024, en donde que estima una baja sin precedentes del 27 % en un año en las muertes por sobredosis. Estas disminuciones son alentadoras y probablemente se relacionaron con una serie de factores, entre los que se incluyen las inversiones en prevención primaria, la salud mental, la reducción de riesgos y los programas de prevención de sobredosis. No obstante, los recortes presupuestarios actuales y propuestos a nivel federal, la reducción de la fuerza laboral de la salud pública y la reorganización propuesta de las agencias federales probablemente perjudiquen este avance, según un nuevo informe.
El informe Pain in the Nation 2025: the Epidemics of Alcohol, Drug, and Suicide Deaths (Dolor en el país 2025: la epidemia de muertes por alcohol, drogas y suicidio), que hoy publica Trust for America’s Health, expone que la cantidad conjunta de decesos a causa del alcohol, las drogas y los suicidios en los Estados Unidos disminuyeron en 2023 por segundo año consecutivo, tras dos décadas en las cuales tales decesos aumentaban a un ritmo alarmante. Aun así, más de 200.000 estadounidenses murieron a causa de sobredosis por alcohol, drogas o suicidio en 2023, el doble de la tasa por tales causas de muerte de hace 20 años atrás.
Estos nuevos datos ponen de manifiesto el valor de la inversión en salud mental y en los programas de prevención de consumo de sustancias como, por ejemplo, garantizar el acceso a los servicios correspondientes de salud mental, trastorno por consumo de sustancias e intervención por crisis, acceso a medicamentos que revierten la sobredosis, y la inversión en la salud mental y la resiliencia de los niños. No obstante, en los datos también se observa que se necesita hacer mucho más para garantizar que el avance contra las muertes a causa del alcohol, las drogas y el suicidio se mantengan, además de que las disminuciones logradas respecto a tales decesos están produciéndose en cada una de las comunidades y entre todos los grupos poblacionales.
“Los datos demuestran que en las décadas de inversión y desarrollo de capacidades con respecto a la prevención del consumo de sustancias, los programas de reducción de riesgos y los servicios de salud mental ayudaron a disminuir las muertes relacionadas con este flagelo. Actualmente, el desafío consiste en basarse en estas inversiones y mantener este avance. Con estos programas se salvan vidas, y no se debería recortar su financiamiento”, declaró Nadine Gracia, M.D., MSCE, presidenta y directora general de Trust for America’s Health.
Las tasas de sobredosis por drogas disminuyen, pero aún estamos en niveles trágicos.
En 2023, 105.007 estadounidenses en todo el país murieron a causa de sobredosis por drogas. Tras los aumentos precipitados en la tasa de muertes por sobredosis en 2020 y en 2021, la tasa general de mortalidad por sobredosis en 2022 no se modificó prácticamente y la tasa de mortalidad en 2023 fue un 4 por ciento menor. Los datos de mortalidad provisorios durante 2024 indican una disminución sin precedentes en un año del 27 por ciento en las muertes por sobredosis a nivel nacional. Se observaron en siete estados (Luisiana, Michigan, New Hampshire, Ohio, Virginia, West Virginia, y Wisconsin) y en Washington D.C. las disminuciones más importantes al tener bajas del 35 por ciento o más en muertes por sobredosis durante el año.
Según expertos en salud pública, los sistemas de datos mejorados que permiten hacer un seguimiento en tiempo real del consumo de sustancias y sus efectos, la ampliación y la eficacia de estrategias de prevención de sobredosis como los programas que garantizan el acceso a la naloxona y a la buprenorfina, o herramientas de control de drogas, tuvieron en conjunto un papel importante en la baja de las tasas de mortalidad.
No obstante, la mejora no fue uniforme en todos los grupos poblacionales ni regiones del país. En 2023, la población blanca fue el único grupo poblacional que tuvo una disminución estadísticamente significativa con respecto a las muertes por sobredosis de drogas; otros grupos poblacionales tuvieron cambios poco significativos o aumentos. Las tasas de muerte por sobredosis de drogas en 2023 fueron las más altas en los grupos poblacionales indoamericano y nativos de Alaska (AI/AN) (65 muertes por cada 100.000 habitantes), en adultos de 35 a 54 años (57,3 muertes por cada 100.000 habitantes), en la población de color (48,5 muertes por cada 100.000 habitantes), y en los hombres (45,6 muertes por cada 100.000 habitantes).
Disminución de las muertes inducidas por el alcohol
En 2023, 47.938 estadounidenses murieron por causas inducidas por el alcohol. La tasa general de mortalidad inducida por el alcohol ajustada por edad disminuyó en un 7 por ciento de 2022 a 2023 (de 13,5 a 12,6 muertes por cada 100.000 habitantes). Esta reducción se acumuló a un 6 por ciento de disminución del año anterior y atravesó a casi todos los grupos demográficos y geográficos, aunque dichas muertes aún afectan de manera desproporcionada a determinados grupos. Las tasas de muerte inducidas por el alcohol en 2023 fueron las más altas en los grupos poblacionales IA/NA (61,5 muertes por cada 100.000 habitantes), en adultos de 55 a 74 años (32,5 muertes por cada 100.000 habitantes), en adultos de 35 a 54 años (20,2 muertes por cada 100.000 habitantes), y en los hombres (18,1 muertes por cada 100.000 habitantes).
Sin cambios en las muertes por suicidio
La tasa de mortalidad general por suicidio en los Estados Unidos sigue prácticamente igual de 2022 a 2023 (14,2 y 14,1 muertes por cada 100.000 habitantes, respectivamente). En 2023, 49.316 estadounidenses murieron por causas del suicidio. Las tasas de muerte por suicidio ajustada por edad en 2023 fueron las más altas en los grupos poblacionales AI/AN (23,8 muertes por cada 100.000 habitantes), en los hombres (22,7 muertes por cada 100.000 habitantes), y en los adultos de 75 años o más (20,3 muertes por cada 100.000 habitantes).
La cancelación de presupuestos y los recortes futuros en los programas de prevención costarán vidas
Si bien con estos datos se demuestran avances reales, la comunidad de la salud pública se encuentra unida en esta preocupación con respecto a los cambios en los avances debido a los recortes en la inversión federal relacionados con la promoción de la salud, la intervención en situaciones de crisis y los programas de prevención de sobredosis. Por ejemplo, el personal y la financiación del Centro de Lesiones de los CDC sufrieron una reducción drástica y se ha propuesto eliminar al Centro en la solicitud de presupuesto del gobierno para el año fiscal 2026. El Centro de Lesiones lleva a cabo investigaciones y recopila datos. Aproximadamente, el 80 por ciento de su financiación se destina a los estados y demás entidades para la prevención de sobredosis, suicidios y experiencias infantiles negativas (ACE).
Asimismo, la Administración de Servicios de Salud Mental y Abuso de Sustancias (SAMHSA) ha sufrido importantes reducciones en su dotación de personal, lo que incluyó personal que trabajaba en la Línea 988 de atención al suicidio y situaciones de crisis y un potencial recorte de presupuesto de 1,07 mil millones para el año fiscal 2026. El gobierno propuso incorporar a los programas que queden de la SAMHSA y del Centro de Lesiones en la nueva Administración para unos Estados Unidos Saludables. Estas acciones siguieron a la recuperación del gobierno de miles de millones de dólares de financiación a la salud pública que ya estaban en marcha en los estado y comunidades de todo el país, incluida la prevención del suicidio.
En el informe Pain in the Nation, se llama a una inversión constante en los programas de prevención y reducción de riesgos y se incluyen recomendaciones sobre medidas que los representantes políticos a nivel federal y estatal deberían tomar, entre las que se incluyen:
- Proteger y apoyar las inversiones en los sistemas de salud pública y conductual y en programas de prevención de lesiones y violencia a fin de mejorar la salud mental y el bienestar de todos los ciudadanos de los Estados Unidos;
- Seguir mejorando los sistemas de datos, como Datos de sobredosis para la acción de los CDC, para hacer el seguimiento de las tendencias emergentes según las métricas geográficas, demográficas y por tipo de droga con el fin de orientar las respuestas a nivel local, estatal y nacional y prevenir casos de sobredosis y muertes en tiempo real;
- Enfocarse en las causas subyacentes de los trastornos por consumo de sustancias por medio de la intervención temprana y políticas de prevención incluidos los programas de ampliación de resiliencia y prevención de consumo de sustancias en las escuelas y aumento del acceso a servicios sociales y de salud mental para los niños y sus familias;
- Maximizar las estrategias de reducción de riesgos y los tratamientos de trastornos por consumo de sustancias a fin de disminuir el riesgo de sobredosis, y dar apoyo a las iniciativas para limitar el acceso a medios fatales de suicidio;
- Respaldar la continuidad de los programas de intervención de crisis y ampliar la dotación de personal para que brinde tratamiento de salud mental y por consumo de sustancias; Desarrollar la capacidad en la comunidad para garantizar el acceso a los servicios de salud mental y consumo de sustancias para todos los que necesiten estos servicios.
Lea el informe completo en: https://www.tfah.org/report-details/pain-in-the-nation-2025/
Trust for America’s Health es una organización sin fines de lucro no partidaria relacionada con políticas, investigación y defensa de la salud pública que fomenta la salud óptima para cada una de las personas y comunidades, y prioriza la prevención de enfermedades y lesiones a nivel nacional.
